February 14, 2013
A Primer of Hyperbaric Therapy
for Parents
By K Paul Stoller, MD, FACHM, Chief
of Hyperbaric Medicine Amen Clinics
Adjunct Assistant Professor, AT Still University School of Medicine
Since 2004, Hyperbaric Oxygen has been
a frequent topic discussed at autism conferences and physician
education events. This document outlines the treatment, research
and information for parents.
Overview
Hyperbaric Oxygen Therapy (HBOT) works
as its name implies – hyper (more of) and baric (pressure)
and in fact that is how it works. It is the increased pressure
of the gas we breathe everyday that can actually signal the DNA
in our cells to perform healing tasks that the body normally
can’t do.
Ground zero for this activity is the mitochondria,
which are the little organelles inside of our cells that convert
oxygen and sugar into the gasoline the cells run on (ATP) –
this is called cellular respiration. It doesn’t take much
to knock mitochondria off-line and then that cell can’t
perform the job it was assigned. So, be it oxygen deprivation,
external toxic exposure, or a hyper-immune reaction to an infection
or a vaccine the mitochondria will be damaged.
We know how Hyperbaric therapy works –
it works by reviving the little mitochondria and actually causes
mitochondrial biogenesis, so that if you need more mitochondria
in your neurons more of them will form. It is interesting to
note that the reason the ketogenic diet helps patients with certain
types of neurological problems is that ketone bodies help support
mitochondrial function. My opinion is that hyperbaric therapy
is the most effective way to do this. It is that simple –
this is not rocket science, but it is non-invasive brain repair.
As long as supportive biomedical interventions
are taking place at the same time, be that detoxification, the
appropriate diet for that child (GF/SF/CF, the SC diet or the
GAPS diet, etc.), the appropriate supplements are on board, (folinic
acid, B12, ALA, glutathione, etc.), foods the child is allergic
to are eliminated and any infectious issues are being dealt with
(such as yeast, viral load, Lyme, Mycobacterium, etc.) then hyperbaric
therapy can commence. Hyperbaric therapy is not a substitute
for a comprehensive bio-medical intervention strategy, and again
alone it is not a cure, but it can be an important addition to
the overall treatment plan.
Hyperbaric therapy is perhaps the safest
procedure in medicine at the pressures used to treat brain injuries
and children on the spectrum.
What are Hyperbaric Chambers?
There are many types of hyperbaric chambers
in all shapes and sizes, but they are not all equal. The term
“hard-shell” chamber refers to chambers made of steel
and acrylic that can achieve pressures equal to three atmospheres
and beyond. There chambers that are small one person monoplace
devices all the way up to submarine sized 30 person multiplace
chambers. The hard-shell chambers can be compressed with 100%
oxygen or room air, but if they are compressed with room air,
as all multiplace chambers are, there are oxygen hoods or masks
given to the patient(s) so they can breathe in the enriched oxygen.
The “soft-shell” or portable
chambers come in all sizes as well, but the largest of the group
are approximately seven feet long and 33 inch in diameter. They
only inflate to 1.3 atmospheres (under current FDA regulations),
which is about 12 feet of seawater pressure (the pressure you
would feel if you were swimming 12 feet below the surface of
the water). Soft-shell chambers can have oxygen pumped into the
chamber by an FDA licensed oxygen concentrator, but even 1.3
atmospheres of compressed room air will increase the partial
pressure of oxygen by almost 50%. Oxygen concentrators will increase
the oxygen level but this varies based on if the patient wears
or does not wear a mask.
Which pressure is best and is more oxygen
better?
There is a therapeutic window that most
brain injuries respond to and that is 1.3 to 2.0 atmospheres.
There are always exceptions and special cases, but pressures
between 1.3 and 1.5 atmospheres seems to be the sweet spot for
the utilization of glucose by the brain and so this is a target
pressure for many protocols that treat brain injuries.
More pressure and more oxygen are not better.
The pressurized air (which contains more oxygen because of the
increased pressure) or 100% pressurized oxygen act as signaling
agents to as many as 8000 genes. The mitochondria have their
own DNA and this is where the action takes place to bring back
the energy levels of injured or poisoned brain cells. More genes
are actually signaled at 1.5 atmospheres than at higher pressures.
How does one get treated?
Hyperbaric treatment facilities that are
not connected to hospital operations almost always treat conditions
that have yet to be approved by the FDA – so-called “off-label”
conditions. These free-standing centers are few and often far
between, and since the brain injury protocol requires daily treatments
for months; both treatment cost and distance to the nearest clinic
become critical matters.
Optimally, you will want your child to
be treated at a clinic that has experience treating children
with brain injuries and where there is a physician with experience
in treating children on the spectrum. That is the best case scenario,
but that situation is not widely available. The second best option
is to start off at such a center and then rent a portable chamber
or buy one, as most do who start off renting a chamber.
Portable chambers go to 1.3 atmospheres
and are not allowed to be inflated with oxygen; although they
can have oxygen pumped in at 10 liters per minute by and FDA
licensed oxygen concentrator. Not every child will be a responder
at the low pressure, but most will respond. For the vast majority
of affected children, the best case and even the second best
case options are not practical, which makes having a portable/soft
chamber at home the only real treatment option.
How many treatments are required?
Hyperbaric oxygen therapy is prescribed
by a physician based on that patient’s need. Typically for
Autism Spectrum issues combined with other co-morbid medical
conditions therapies are typically prescribed in 1 hour increments
once full pressure is obtained. Treatment length varies by case.
Typically treatments are between 20 – 80 separate appointments.
Hyperbaric oxygen therapies are more efficacious to be performed
in sequential days.
Doctors will work with patients to evaluate
individual needs and come up with a treatment plan. Each treatment
plan varies. This therapy could be prescribed in groups. For
example, a doctor may prescribe three separate 20 treatment sessions
as part of a treatment plan. Please check with your doctor for
additional details.
What chamber is the right chamber?
As I have already pointed out there are
many shapes and sizes, but not all portable chambers are equal.
There are some very cheaply made chambers on the market and so
a parent is best served by a manufacture that has the best guarantee,
the best system for fixing a chamber should something go wrong,
and has a long track record in the USA of selling their chambers
from the same location. In other words, an established company
that stands behind their product is best and what is not best
is looking for the best price. There is only one company I know
of that will both rent chambers and buy back their chambers to
refurbish them and sell them at a reduced price – there
is only one chamber manufacture in the USA that sells a portable
chamber that is Pressure Vessel Certified – that is the
only company I would obtain a chamber from.
But isn’t hyperbaric therapy controversial?
Indeed it is but the controversy is political
not scientific. When Canadian (Quebec) parents petitioned their
reluctant government to fund a study examining the use of hyperbaric
oxygen to treat children with cerebral palsy, the government
put in place a man who designed the study to confuse. He removed
the control group and only looked at two treatment arms: 1) children
receiving hyperbaric oxygen at 1.75 atmospheres; 2) children
receiving hyperbaric air at 1.3 atmospheres.
The results of the study showed that Gross
Motor Function improved 15 times greater with treatment than
with previous therapies – both groups of children. Eighty
percent of the children involved in this Canadian study (Lancet
2002), and there were 110 children, improved including improvement
in cognition, speech and other outcome measures. So, what did
the amoral representative of the Canadian government do who was
sent in to obfuscate the results of the study? He called the
1.3 atmosphere group a placebo group (he did this in French only
– in English he called it a sham treatment) and then he
announced hyperbaric therapy didn’t work because the treatment
group’s results were no different than the placebo group.
Since few physicians and scientists know
anything about hyperbaric medicine, there was no one around to
point out that 1.3 atmospheres is hardly a placebo when it increases
the partial pressure of oxygen by almost 50%. But they knew that
– this was all about making sure the government didn’t
have to pay for this therapy for handicapped children and it
has worked to this day. Children with CP can not receive hyperbaric
therapy from most 3rd party payers in part because of the propaganda
surrounding this ten year old study.
The truth is that 10 times more progress
was made during the two months of hyperbaric therapy (while all
other therapies were ceased) than during the three months of
follow-up with OT/PT restarted.
In 2005, I published an article in the
journal PEDIATRICS showing that hyperbaric oxygen therapy could
reverse the brain damage caused by Fetal Alcohol Syndrome (FAS).
That article was met with resounding silence. FAS is the most
common from of non-hereditary mental retardation and is considered
to be incurable and untreatable.
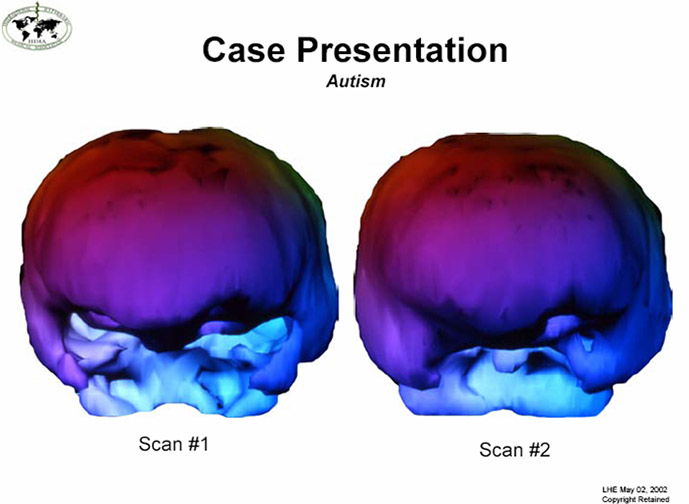
Below are functional brain images of what
hyperbaric oxygen can do for a child on the spectrum before and
after treatment.
This is a functional brain scan called
a SPECT scan. You are looking at the front of the brain. Before
hyperbaric oxygen was administered there is little to no activity
in the temporal lobes and lack of blood flow to the prefrontal
cortex. After treatment the horns of the temporal lobes can be
seen now and the deficits in the prefrontal cortex are filling
in. (The scans were done by Paul Harch, MD, Director of the LSU
Hyperbaric Medicine Fellowship and were submitted into the Congressional
record.)
Should I ask my doctor about clinic
treatments or in home?
Many MAPS Doctors and the International
Hyperbaric Association (IHA) recommend the first hyperbaric oxygen
treatments occur in person, with a supervising physician, trained
medical staff at 100% oxygen.
What if I want to buy or lease a hyperbaric
chamber for in home use?
Should parents and treating physicians
recommend additional hyperbaric treatments utilizing a home unit
IHA will refund a partial credit towards the purchase or a unit.
The partial credit is available when patients visit an IHA center
only.
The IHA member benefit (i.e. if you go
to an IHA center and receive in patient HBOT services, you can
apply a “credit” to a purchase of a chamber –
if you choose to purchase.)
Read updated studies and research information.
For additional providers – please
visit www.hbotproviders.com
It is recommended family’s consult
their doctor (MAPS! doctors, especially) for recommended HBOT
providers. Having knowledge about working with children on the
autism spectrum is important.
A Final Note
Hyperbaric therapy requires a physician’s
prescription to utilize a hard shell chamber or to buy a portable
or to receive therapy at a hyperbaric clinic. The child must
be able to equalize the pressure in the middle ear by swallowing,
even at the low 1.3 pressure level
Studies about Hyperbaric oxygen and
autism:
|
1. |
Hyperbaric
treatment for children with autism: A multicenter, randomized,
double-blind, controlled trial. Rossignol DA, Rossignol LW,
Smith S, Schneider C, Logerquist S, Usman A, Neubrander J, Madren
EM, Hintz G, Grushkin B, Mumper EA. BMC Pediatr. 2009 Mar 13;9:21.
PMID: 19284641 [PubMed - indexed for MEDLINE] |
|
|
|
2. |
Hyperbaric
oxygen therapy in Thai autistic children. Chungpaibulpatana
J, Sumpatanarax T, Thadakul N, Chantharatreerat C, Konkaew M,
Aroonlimsawas M. J Med Assoc Thai. 2008 Aug;91(8):1232-8. PMID:
18788696 [PubMed - indexed for MEDLINE] |
|
|
|
3. |
A
review of recent reports on autism: 1000 studies published in
2007. Hughes JR. Epilepsy Behav. 2008 Oct;13(3):425-37. Epub
2008 Jul 31. Review. PMID: 18627794 [PubMed - indexed for MEDLINE] |
|
|
|
4. |
The
effects of hyperbaric oxygen therapy on oxidative stress, inflammation,
and symptoms in children with autism: an open-label pilot study.
Rossignol DA, Rossignol LW, James SJ, Melnyk S, Mumper E. BMC
Pediatr. 2007 Nov 16;7:36. PMID: 18005455 [PubMed - indexed for
MEDLINE] |
|
|
|
5. |
Hyperbaric
oxygen therapy might improve certain pathophysiological findings
in autism. Rossignol DA. Med Hypotheses. 2007;68(6):1208-27.
Epub 2006 Dec 4. PMID: 17141962 [PubMed - indexed for MEDLINE] |
Original article:
www.tacanow.org/family-resources/hyperbaric-oxygen-treatment-for-autism...